
It should have been a day of routine maintenance on November 9, 2010 at the DuPont plant in North Tonawanda, New York. Tank 1, which normally contained 10,000-gallons of polyvinyl fluoride (PVF), a slurry used in manufactured countertops, had been cleaned and inspected in preparation for repairs. All relevant procedures had been followed and all paperwork completed. The team performing the work had climbed up to the top of the tank on the catwalk and began grinding and welding to repair the equipment.
However, just a few minutes after 11:00 am, an explosion blew the steel cover from the tank. A worker was killed, and nearby residents felt the blast from nearly a mile away. Concerned about toxic gases, authorities cautioned residents to immediately close their windows as the cleanup and investigation began.
What caused this disaster?
Incomplete Lockout Procedure. A routine inspection had found corrosion on the hatches of PVF slurry Tanks 1, 2, and 3, and the plant scheduled repairs. In preparation for the repair work, Tanks 1-3 were locked out. This included the fill lines, which prevented any PVF vapors from entering the tanks during the maintenance. The repairs were completed on Tanks 2 and 3, and they were restarted, but repairs on Tank 1 were delayed because certain required parts were unavailable. When the maintenance finally began on Tank 1, the fill lines remained locked out as prescribed by the normal Lockout Procedure. However, an overflow line servicing all three tanks remained open, which provided a path for flammable vapor to migrate from the in-use Tanks 2 and 3 into the locked-out Tank 1.
Lack of Air Monitoring. DuPont personnel had monitored the atmosphere in the tank before allowing the repairs to begin but did not continue to monitor the atmosphere as the work progressed. Air monitoring inside the tank may have alerted the repair team of the hazardous, flammable vapors accumulating in Tank 1.
Insufficient Training and Awareness. Prior to beginning the repairs, the facility issued a “hot work permit” for the work, certifying the area was safe for welding and permitting welding to occur. However, the DuPont personnel who signed it did not fully understand the chemical process around PVF use or the equipment schematics.
Context and effects of the disaster
E.I DuPont de Nemours, typically referred to as DuPont, is on the Fortune 100 list and is one of the world’s largest chemical companies. It provides a wide variety of products and services to consumers and other businesses, which range from electronics and construction to agriculture and apparel. DuPont’s plant in North Tonawanda produces Corian countertops and Tedlar films, which require PVF slurry as an ingredient.
An investigation by the Chemical Safety Board (CSB) found that the explosion was caused by the ignition of flammable vapors within Tank 1. The CSB could not determine the exact source of ignition, but suggested the following three potential sources:
- Excessive heating of the tank walls due to the hot work (welding)
- Sparks from the hot work falling into the tank,
- Flammable PVF vapors escaping the tank and entering the hot work area where they were exposed to sparks.
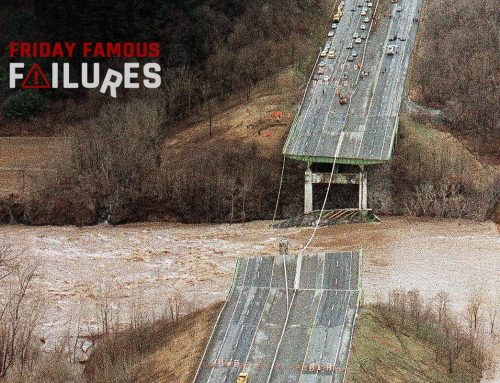
The explosion blasted a large portion of the cover off the tank, which included the large motorized agitator assembly (which normally stirred the slurry). The tank roof segments and wrecked agitator assembly came to rest hanging over the ragged edges of the tank walls by the agitator wiring. The welder died instantly from the blast, and the foreman supervising the repairs suffered first-degree burns but no other major injuries. The fire quickly consumed the flammable vapor and, after the explosion, self-extinguished.
The CSB investigation team made the following recommendations:
- That air-monitoring requirements for hot work include the interior of tanks and other containers, whenever tanks or other containers are part of the equipment on which hot work is being performed
- That DuPont redefine Tanks 1-3 as a single system in their Lockout procedure, requiring all three to be empty of PVF before maintenance is performed
- That DuPont requires all pipes connected to equipment under repair to be positively isolated prior to issuing a hot work permit
The lead investigator of the accident summed up the findings of the investigation as follows:
DuPont’s process hazard analysis incorrectly assumed that vinyl fluoride in the Tedlar process could not reach flammable levels in the slurry tanks. And, critically, DuPont personnel did not properly isolate and lockout Tank 1 from Tanks 2 and 3 prior to authorizing the hot work. The flammable vapor was able to pass through the overflow line into the tank the welder was working on, unknown to him or to the operators who signed off the hot work permit.
After the incident, DuPont improved its corporate hot work authorization procedure and its lockout procedures in accordance with the CSB recommendations. Additionally, DuPont invested $6.8 million in safety upgrades in the North Towanda plant.
On October 1, 2015, the Occupational Health and Safety Administration fined DuPont $724,000 for the explosion, noting that the fine amount was reduced significantly due to the safety improvements DuPont had already made. DuPont was also placed on the “Severe Violator Enforcement Program” and was subject to additional monitoring and auditing by OSHA in the years following the citation.


There is an expression in the Dutch language, which translates roughly as follows: “To fill the pit after the calf has drowned.” In other words taking measures to prevent an incident after an incident has happened in lieu of before an incident. Unfortunately the American culture is better suited to dealing with incidents than with preventing them. This is very clear in the American medical practice. The medical practice in China for example focuses more on prevention, because of the historical practice of killing the medical doctors of the emperor if the emperor fell ill. These doctors were forced to focus on prevention, rather than treatment. They were dead before treatment could even be contemplated.
I worked for Dupont years ago before they pulled out of operating the site I was at. As memory serves me, they were a very safety conscious culture so I was surprised when I read the company name in the header. However, several of the statements in the write-up point to a deeper problem facing all of America industry. An issue which has been written about many times, the retiring workforce. And an issue, which in my opinion, AI is not going to solve. I could be wrong but the phrases “did not continue to monitor”, “personnel who signed it did not fully understand the chemical process ” and “process hazard analysis incorrectly assumed that vinyl fluoride” indicate to me that less experienced personnel were involved in these steps. I am in the demographic where I have experienced age discrimination (ie :I cost too much”). Unfortunately, the $724,000 fine could almost take me to retirement in 2029. Pay me now or pay me later. The preceding comment mentioned the Chinese culture. I have been exposed to several younger non-US coworkers in my career. I have found that not only the Chinese, but most cultures outside the US value the experience age brings. Hopefully American industry wakes up before it is too late.
One thought is: Did anyone know this could occur? If so, why was the information not shared? (siloed by whom?) By this article it appeared that the CBS had no idea this could happen or how it happened and the assumptions went to a shared overflow vent. (highest probability) Still without definitive answers. OSHA appears to see a cash cow and fined Du Pont just for the $$$ and provided zero comment or protocols for the prevention of future occurrences. OSHA took the results of the CBS and ran. Du Pont did a lot more to reduce or eliminate future happenings than either the CBS or OSHA.
Just reading the writeup, based on my experience overflow lines and or pressure relief lines are typically designed with no means of shutting down for safety reasons. Some designers save money by combining these items when multiple tanks are installed no matter for what process / system. Dedicated lines for each tank would have added a few dollars, however taking items out of service and or maintenance should always be considered.